Pessary therapy for prolapse and urinary incontinence is much better than its reputation suggests! Gone are the days when pessaries caused foul-smelling discharge, infections, and ulcerations. This traditional treatment method has returned with more modern, much more comfortable pessary designs made of special silicone developed specifically for pessary therapy.
This resurgence is also due, not least, to the sobering results of prolapse and incontinence surgeries. The long-term outcomes are far from what most surgeons had expected.
"More than 20 years of experience in the development and production of pessaries form the basis for quality and cost-effectiveness at our company."
Uterine prolapse is usually a consequence of obstetric injuries or a congenital weakness of the connective tissue. The uterine ligaments and the supporting pelvic floor muscles are no longer able to perform their function. The uterus descends, leading to feelings of pressure and back pain, chafing, ulcers, and bleeding. A urethrocele, cystocele, or rectocele often occurs with prolapse. A urethrocele promotes stress incontinence because the urethra opens in a funnel shape during straining.
A cystocele, especially if it prolapses, can kink the urethra and consequently cause micturition problems and urinary retention; and a rectocele finally causes defecation problems.
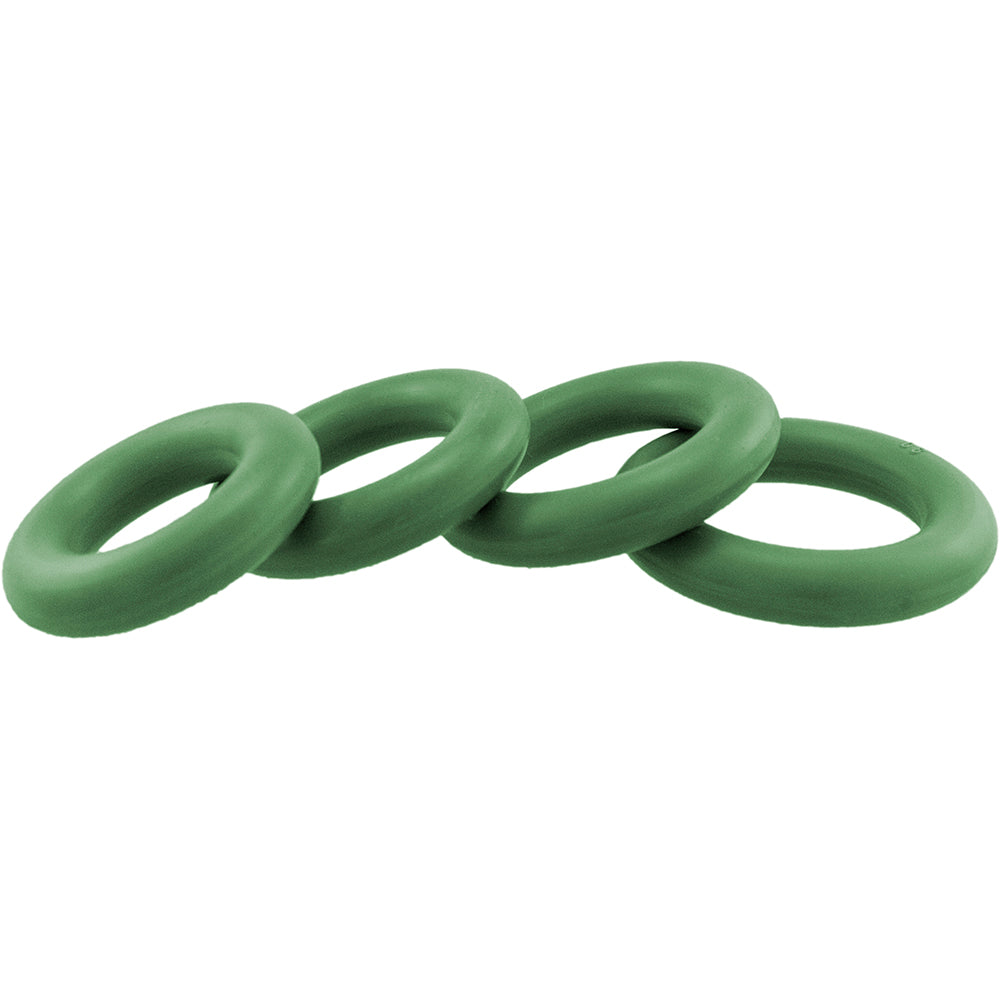
Various types of pessaries have proven effective in treating urinary incontinence and prolapse: the urethral pessary, the cube pessary, the ring pessary, and the sieve-bowl pessary.
The ring pessary is used for prolapse and stress incontinence, but also to prepare for prolapse surgery and to loosen scar tissue (z.B. (after vaginal wall repair). The cube pessary is used to treat uterine prolapse, descent without urinary incontinence, cystocele, rectocele, and scar tissue loosening.
The urethral pessary rests on the medial portion of the levator ani muscle. This pessary repositions the prolapsed urethra and also shifts the proximal urethra ventrally and superiorly, thus reducing the occlusion pressure. Significantly improved. However, if the levator ani muscle is weak and insufficient, the ring pessary will not stay in place. Therefore, if it doesn't stay in place for a woman with stress incontinence, you can switch to a cube pessary.
This type of pessary is based on a different principle of action, as cube pessaries adhere to the vaginal wall like suction cups. This results in stabilization and firmness. Cube pessaries also replace all other "special constructions" of earlier times in cases of genital descent and prolapse (with insufficient levator ani).
When a cube pessary is used to reposition a cystocele, it can occasionally reveal underlying stress incontinence. In such cases, a switch to a ring or sieve-shell pessary is necessary.
All patients with cystocele, rectocele, and uterine descent or prolapse should first be treated with cube pessaries before surgery is considered. The smallest cube that still adheres is chosen. After the first and second month of treatment, it is usually possible to switch to a smaller cube each time.
In over a third of cases, permanent repositioning (without a pessary) is achieved after 3-5 months; surgery is unnecessary. However, in the remaining patients, where permanent repositioning and satisfactory symptom relief are not achieved despite bladder and pelvic floor exercises and local estrogen therapy, surgery is unavoidable.
Of course, there's nothing wrong with lifelong pessary therapy.Since the patients remove the cube pessary in the evening and reinsert it in the morning using Ladysoft as a lubricant, good tissue relief and hygiene are ensured.